Apples and oranges: biomarkers and SCr
다른 의학의 분야들 (소화기내과, 심장내과, 종양내과 등) 은 급성 질환을 평가하는 여러가지 도구들이 있지만 신장내과의 경우 single assay 에 대체로 의존하는 모습이 있다.
NGAL and KIM1 : provide an assessment of cell stress and damage, tubular injury biomarkers (cell viability)
SCr and cystatin C : provide an assessment of steadystate kidney function (kidney function)
–> 이 두 가지 파라미터의 변화는 동시에 / 또는 연속적으로 / 또는 독립적으로 일어날 수 있다.
Loss of kidney function may or may not be the result of kidney injury
Kidney injury may or may not cause loss of kidney function.
–> Cardiology 의 Troponin (myocardial infarction) 과 Echocardiography (congestive heart failure) 사이의 관계와 유사하다.
이러한 2가지 종류의 평가방법을 서로 가장 잘 이용하는 방법은 아마도 연속적으로 보는 것이다.
그 이유는 kidney injury must occur in stages
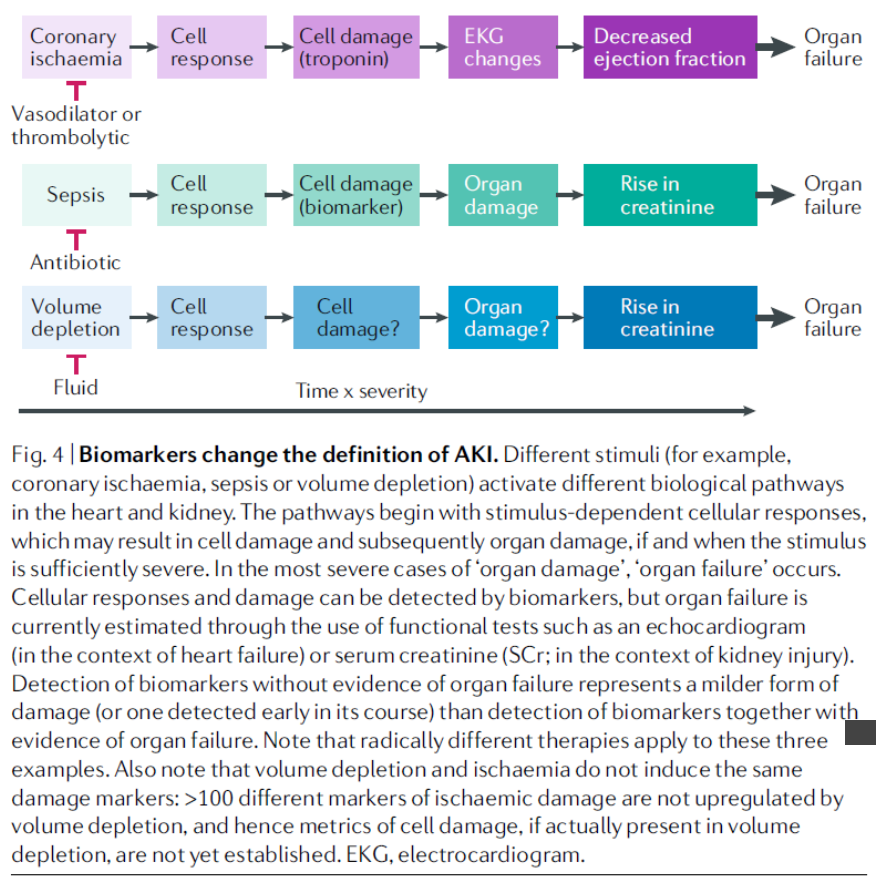
Damaging stimuli (for example, sepsis, obstruction or nephrotoxins)
–> sequence of events : cellular responses [assessing metabolomic responses] + cellular damage [ assessed by measurement of transcriptomic responses and biomarkers ]
–> widespread organ damage + organ dysfunction (as determined by changes in steadystate
markers of kidney function)
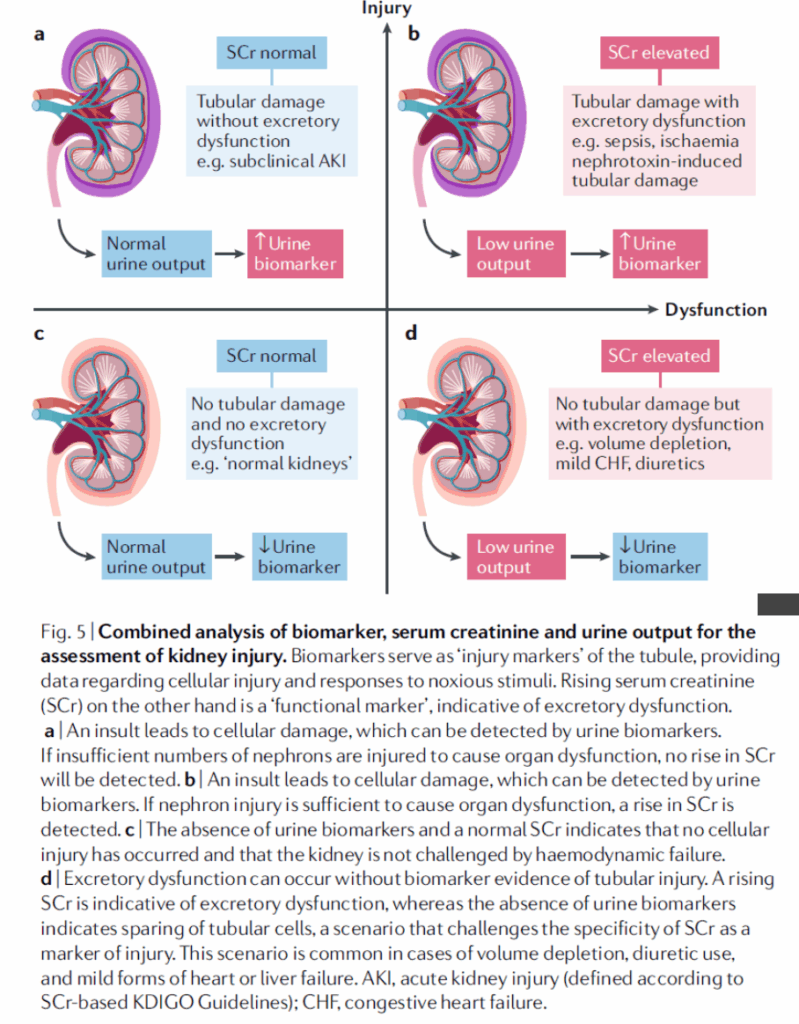
a. )
expression of injury biomarkers increases
without a rise in SCr
Ex. ) initial phase of damage, damage is not sufficiently widespread to cause loss of excretory function
b. )
expression of biomarkers is accompanied by a rise in SCr level
Ex. ) context of tubular damage that is sufficient to cause loss of excretory activity
d. )
rise in SCr occurs
without increased expression of kidney injury biomarkers
Ex. ) following activation of a pathway that reduces kidney excretion without changing known tubular injury biomarkers, reversible volume depletion
* 참고로, subacute AKI, subclinical AKI 라는 개념은 여기 그래프에서는 들어가지 않는다.
–> 왜냐하면, biomarkers are simply expressed more rapidly and are more sensitive indicators of injury than is SCr.
* “subtypes of AKI” 라는 개념의 different causes of elevated SCr 라는 서술도 부적절하다.
–> 왜냐하면, different injurious stimuli 가 different biological processes 를 유발시키는데, 서로 관련이 있을 수도 있고, 없을 수도 있고, functional loss 를 유발할 수도 있고 유발시키지 않을 수도 있기 때문이다.
Since biomarkers provide information that is distinct from that provided by SCr
–> combined analysis of biomarkers and SCr can have clinical benefits
* 예 ) 지난 연구 예시
– NGAL and SCr 을 조합하여 RRT, 중환자실, 입원기간, 사망률 risk 를 나누어 예상할 수 있음을 보여주는 연구
– NGAL or KIM1 with SCr 을 조합하여 7일내 RRT 또는 사망율 예측을 15% 의 경우에서 할 수 있었으나, Biomarker 혹은 SCr 단독으로 사용하였을 경우에는 5% 의 경우밖에 예측할 수 없었던 연구
– NGAL and cystatin C 을 조합하여 severe AKI 를 예측하고 동시에 possibility of ‘transient AKI’ 를 배제했던 연구
–> Elevation of a functional marker without the finding of urinary NGAL 의 경우 excellent predictor of ‘transient AKI’ 이었다.
This scheme enables the diagnosis of acute tubular injury to be categorized into two potentially simple ideas:
– first, evidence of injured cells derived from non-invasive biomarkers
– second, evidence of loss of kidney excretory function based on changes in SCr and/or urine output.