Uses in antifungal agents
1. Propohylaxis
; all patients with neutropenia (before infection)
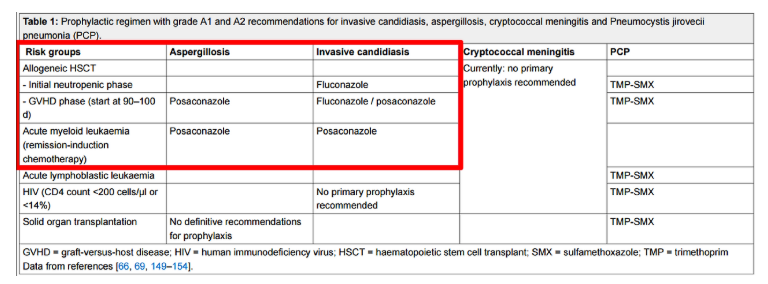
2. Pre-emtive or empirical
; Persistent neutropenic fever + alpha (Galactomannan?, Beta-glucan?, PCR?, HRCT?)
* Empirical Tx. 를 시작하는 경우
1) High risk patients with prolonged neutropenia (10일 이상)
2) Febrile after 4~7 days of broad-spectum antibiotic Tx.
* Pre-emptive Tx. 를 시작하는 경우
1) High risk patients with prolonged neutropenia (10일 이상)
2) Febrile after 4~7 days of broad-spectum antibiotic Tx.
3) + Any of surrogate markers
– Chest or sinus CT
– Galactomannan assay, beta-D-glucan assay
– Recovery of fungi such as Candida or Aspergillus from any body site
** Surrogate markers for invasive fungal infections
| Fungus | Galactomannan | 1,3-beta-D-glucan | PCR (국내에서 활용미흡) |
| A. fumigatus | ++ | ++ | + |
| Non-fumigatus Aspergillus | + | + | + |
| Fusarium | + | + | + |
| Zygomycetes | – | – | + |
| Candida | – | ++ | + |
| Cryptococcus | + | ± | + |
| Penicillium | + | + | + |
| Pneumocystis jirovecii | – | ++ | + |
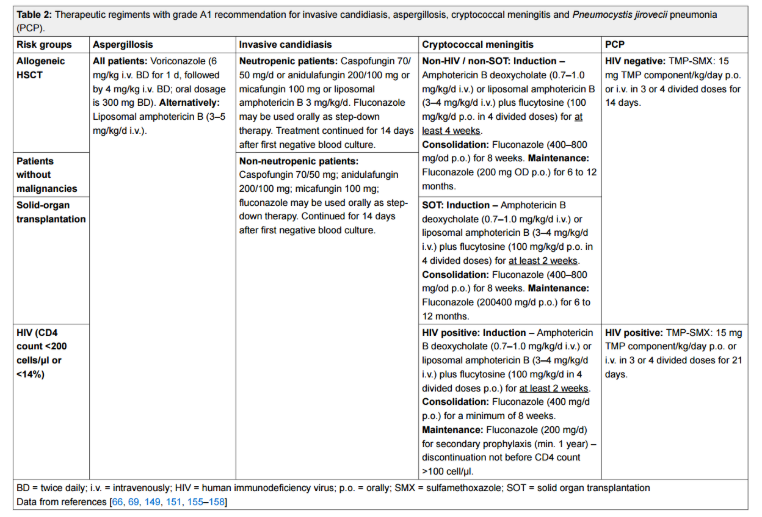
3. Pathogen-directed Tx.
; Persistent neutropenic fever + Culture or pathology
1) Invasive candidiasis
* Primary therapy 는 Echinocandin 을 사용한다.
(alternative therapy 로 Oral or IV fluconazole 을 사용한다.)
※ 예외 ) CNS (LAmB +- 5-U), Eye (Fluconazole/Voriconazole or LAmB), UTI (Fluconazole or AmBd) 일 경우 Primary Tx. 로 Echinocandin 을 선택하면 안된다.
* Echinocandin 에서 Fluconazole 로 변경할 수 있는 기준
- (1) 임상적으로 stable 할 때
- (2) Fluconazole 에 Susceptable 한 균주여야 한다.
- (3) Triazole 에 이전에 노출력이 없어야 한다.
- (4) anti fungal Tx. 이 후 f/u blood culture 가 반복적으로 negative 여야 한다.
* Candidemia 때의 general recommendation
- (1) 중심정맥관을 제거해야 한다. (strongly recommended for non-neutropenic patients → 면역저하자의 경우 중심정맥관 등이 origin 이 아니라 구강에서 왔을 수 있기 때문에 중심정맥관을 save 할 수도 있다.)
- (2) Dilated ophthalmological examination (모든 환자들에게, 진단 후 1주 이내에 → Candida endophthalmitis 확인)
- (3) Follow-up Blood culture : Every day or Every other day until candidemia has been cleared
→ f/u blood culture 를 꼭 나가야하는 대표적인 균주로 MRSA 와 Candidemia 가 있다고 배웠었다. - (4) Duration of therapy
- – Metastatic complication 이 없다면 혈액배양에서 균이 음전된 후 최소 2주 이상 사용.
- – Candida endophthalmitis 가 있다면 최소 4~6주 이상, 안구 병변이 호전될때 까지.
* Invasive candidiasis 때의 항진균제 약제간의 장단점
(1) Polyene
– 장점 : Broad-spectrum / Fungicidal / Good CNS/EYE penetration (LAmB)
– 단점 : Toxicity (nephrotoxicity, infusion-related)
(2) Triazole
– 장점 : oral form (유지요법으로 유용) / TDM / Good CNS/EYE penetration
– 단점 : Limited activity to C. krusei, C. glabrata / Fungistatic / Drug interaction / Dose adjustment in Renal failure
(3) Echinocandin
– 장점 : Fungicidal / No Dose adjustment in Renal failure
– 단점 : Limited activity to C. parapsilosis / Poor CNS/EYE penetration
* 참고 : Esophageal candidiasis
→ 내시경 소견만으로 조직검사 없이 진단이 가능하다.
→ 치료로는 Fluconazole 을 2~3주 사용한다. (좋아졌다고 일찍 중단하지 않는다.)
→ Fluconazole 을 못쓸경우 micafungin 등을 사용가능하다.
→ HIV 검사를 시행한다.
2) Invasive Aspergillosis
* Primary therapy 는 Voriconazole 을 사용한다.
(alternative therapy 로 우선적으로 Liposomal AmB, Isavuconazole (국내에서 아직 사용 못함) 을 사용할 수 있으며, salvage Tx. 로 ABLC, Caspofungin, micafungin, Posaconazole, Itraconazole 등을 사용해볼 수 있다.)
* Primary combination Tx. 는 Voriconazole + Echinocandin 이나 routine 한 사용이 추천되지는 않는다.
3) Mucomycosis
* Primary therapy 는 Liposmal AmB or ABLC + Surgery (수술을 해야한다.)
(Alternative therapy 로 Posaconazole (국내에서는 보험 급여 안된다.) 또는 combination Tx. (Liposomal AmB + [Caspofungin or posaconazole]) 을 시행해 볼 수 있다.)
* Maintenance therapy 로는 Posaconazole 을 사용한다.
4) Cryptococcosis
* 3-phase 로 나뉜다.
* Induction therapy : AmB + Flucytosine (2 weeks)
* Consolidation therapy : Fluconazole (400~800 mg/day for 8 weeks)
* Maintenece therapy : Fluconazole (200-400 mg/day for 6~12 months)
※ 항진균제 antifungal agent 시리즈
- 2023.04.06 – 항진균제 Antifungal agents (1) : 항진균제의 종류, Polyenes, Amphotericin B, Azoles, Triazoles, Echinocandins, Flucytosine, 항진균제의 내성
- 2023.04.07 – 항진균제 Antifungal agents (2) : 항진균제의 종류별 특징, Amphotericin B, Azoles, Echinocandins, 5-FC, 부작용
- 2023.04.08 – 항진균제 Antifungal agents (3) : 항진균제의 사용, 예방적, 경험적, Invasive candidiasis, Esophageal candidiasis, Invasive Aspergillosis, Mucomycosis